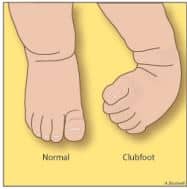
Clubfoot is a congenital deformity where the foot is rigidly turned inward and downward, and is misshapen like a club. It can range from mild and flexible to severe and rigid. One or both feet may be affected. The calf muscle and foot may also be slightly smaller than normal.
Clubfoot is the most common deformity of the bones and joints in newborns. The cause of clubfoot is not exactly known, but it is most likely a genetic disorder and not caused by any action nor lack of action the parents took. It occurs in about 1 in 1,000 babies. If a family already has a child with clubfoot, the risk of having a second child who also has clubfoot increases to 1 in 30.
Treatment starts shortly after birth and consists of a series of manipulations followed by casting that slowly corrects the foot in a specific sequence. This is called the Ponseti Method, name for Dr. Ignacio Ponseti who developed it. Most children will need at least 4 to 6 casts followed by a heel cord release (called the Achilles tendotomy) to help with the final stage of correction.

Casting is performed on a weekly basis. The cast material is soft and may be removed the night before or the morning of the next appointment, allowing the child to be bathed. Prior to casting, the foot is gentlymanipulated. It helps if the baby is as relaxed as possible; the best way to do this is to feed during casting. If you are breastfeeding, consider pumping and bringing in a bottle.
At 4 to 6 weeks, the child’s foot is usually ready for the final stage of treatment – a heel cord release. This is a same day procedure performed in the hospital under general anesthesia. It involves cutting the Achilles tendon to allow the foot to dorsiflex. If this is not done, and the foot is forced up, the arch of the foot may break down. After the heel cord release, one final cast is applied and left on for 2 to 4 weeks. The infant’s heel cord heals very quickly, and the surgery will not cause any permanent weakness.

Bracing is started after the final cast is removed. The Mitchell shoes with a Ponseti Bar is our preferred brace for clubfoot treatmeant because it is comfortable and easy to use. It is extremely important that the brace fits properly and is worn as directed. Studies have repeatedly shown that the success of treatment is deoends on proper use of and compliance with brace wear.
The brace is worn full time (24 hours except for bathing) for 3 months and then worn at naps and night-time until the child is 3 years of age. Following full correction of the clubfoot, clinical visits will be scheduled every 3-6 months for two years, and then less frequently. Your physician will decide on the duration of bracing depending upon the severity of the clubfoot and the tendency of the deformity to relapse.

Although results are better without the need for extensive bone and joint surgery, 5-10% of infants born with clubfeet have very severe deformities with stiff ligaments that are resistant to the manipulation and casting. These babies need surgical correction once it is clear that any previous attempts to improve the deformity with Ponseti Method has failed.
A child with a clubfoot corrected by the Ponseti Method can be expected to have a close to normal foot. Some minor differences may remain; a treated clubfoot is slightly smaller than a normal foot and there is a slight size reduction in the lower leg muscles. The difference depends on how severe the clubfoot deformity was. A small but insignificant degree of shortening of the leg may also be noticeable.
Children with clubfeet can participate in sports like anyone else. In fact, famous athletes such as Mia Hamm (soccer player), Kristi Yamaguchi (figure skater), and Troy Aikman (pro football player) had clubfeet as children and went on to have very successful athletic careers.