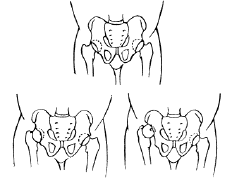
Developmental dysplasia of the hip (DDH) is an abnormality of the hip joint that is present at birth or shortly thereafter. It occurs when the femoral head is not held firmly in the hip socket. The condition is found in babies or young children. The hip may be completely dislocated or the socket may be just a little shallow. One or both hips may be involved.
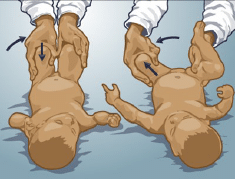
The most common method to identify DDH is a physical exam of the hips. This involves a careful hip examination feeling for any instability, or looseness.
If the infant is at risk for DDH, the pediatrician or orthopaedist may recommend an ultrasound to help diagnose DDH.
Newborns never show any symptoms of DDH. It is painless, however signs of DDH include:
In early infancy, a non-surgical positioning device my be used to needed to keep the hips flexed and abducted. This device is called a Pavlik harness (see picture below). The baby will typically wear the harness for 2 to 3 months or until the instability has resolved and the hip is anatomically reduced.
The patient will be followed for improvement using serial ultrasounds or radiographs ordered by your pediatric orthopaedic surgeon. Your child may be followed for several years. If hip dysplasia is identified in the first few months of life, it can almost always be treated successfully non-operatively. In a few cases, surgery is necessary. Surgery is necessary when measures to reduce the hip are unsuccessful or if the problem is first detected in an older child.
Your doctor diagnoses DDH based on your child’s clinical examination, ultrasound or x-rays. Ultrasound or x-rays may be ordered by your doctor to confirm the diagnosis or to exclude other problems.

No, there is no guaranteed method to prevent a newborn from developing developmental hip dysplasia. However, if diagnosed at a young age, treatment for DDH is successful. When treated appropriately DDH will not cause any difficulties or delays as the child continues to grow and develop. The goal of treating DDH is to prevent the de-velopment of degenerative arthritis of the hip which will otherwise occur in untreated or inad-equately treated DDH.
Developmental hip dysplasia is a congenital deformity of the hip joint present at or shortly after birth that causes one or both hip joints to dislocate. In most cases, hip stability is restored using a non-surgical positioning device.
Developmental dysplasia of the hip (DDH) is an abnormality of the hip joint that is present at birth or shortly thereafter. It occurs when the femoral head is not held firmly in the hip socket. Most often is found in babies or young children, developmental hip dysplasia can affect one or both hip joints.
At Children’s Orthopaedic & Scoliosis Surgery Associates, we have 7 board certified orthopaedic surgeons with fellowship training in pediatric orthopedic care. We understand that when your child is born with a condition like hip dysplasia, it can be a scary and stressful time. Our goal is to treat your child as if they were our own, providing compassionate and expert care from start to finish.
Contact the Children’s Orthopaedic and Scoliosis Surgery Associates for more information regarding treatment options
DDH may cause complete dislocation of the hip joint or the socket may be too shallow resulting in partial dislocation. Common factors that can increase a patient’s risk of having DDH include:
The most common method to determine if a patient is suffering from developmental dysplasia of the hip is a physical exam to determine if the hip joint is instable or loose.
If an infant is at risk for developmental hip dysplasia, the pediatrician or orthopaedist may recommend an ultrasound to help diagnose and confirm the condition. DDH is painless for newborns so they do not show any symptoms, however signs of DDH include:
In addition, the orthopaedic surgeon may order ultrasounds or x-rays to confirm the diagnosis or to exclude other problems.
While there is no guaranteed method to prevent a newborn from developing developmental hip dysplasia, treatment for DDH is successful if diagnosed at a young age. When treated appropriately DDH will not cause any difficulties or delays as the child continues to grow and develop.
The goal of treating DDH is to prevent the development of degenerative arthritis of the hip, which will otherwise occur in untreated or inadequately treated DDH. In early infancy, a non-surgical positioning device, known as a Pavlik harness, is used to keep the hips flexed and abducted. The infant will typically wear the harness for 2 to 3 months, or until the instability has resolved and the hip is anatomically reduced. Some individual patients may need longer bracing periods. Using serial ultrasounds or radiographs, the pediatric orthopaedic surgeon will follow the patient’s improvement closely, up to several years.
If hip dysplasia is identified in the first few months of life, it can usually be treated successfully with a Pavlik Harness. If measures to reduce the hip are unsuccessful or if the problem is first detected in an older child surgery may be necessary.
With 7 fellowship trained pediatric surgeons specializing in orthopaedics and scoliosis, the Children’s Orthopaedic and Scoliosis Surgery Associates team provides state-of-the-art comprehensive care, both surgical and non-surgical, to patients suffering from congenital orthopaedic anomalies, such as developmental hip dysplasia. To learn more about developmental hip dysplasia, please schedule an appointment at one of our Tampa-St. Petersburg locations.