Flatfeet is very common in children; in fact, most children have flat feet and it is considered a normal stage of development. In fact, no child will have much of an arch until the age of three. Most children develop an arch in the first ten years of life if it develops at all, however approximately 20% never develop an arch.
Several studies have shown children who don’t wear shoes develop a better arch than children who wear shoes, but there is no evidence that any type of support, orthotic, shoe or other device can cause an arch to develop. Flatfeet are rarely painful and may run in certain families.
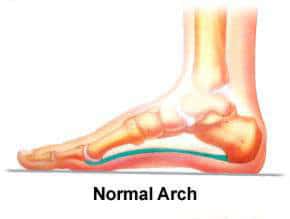
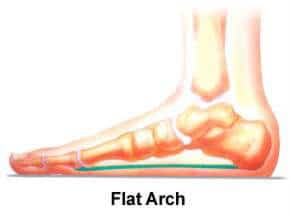
Flatfeet are due to excessive ligamentous laxity (also known as “double jointed” or “loose jointed”). Basically, the tissues that connect and surround the joints – ligaments and capsules – are “loose” which allows the joints to move with more flexibility. This causes the foot to flatten out when the patient is bearing weight (i.e., when standing).
Flatfeet usually appear normal when the child is seated or standing on their toes, but the arches disappear when the child stands properly.
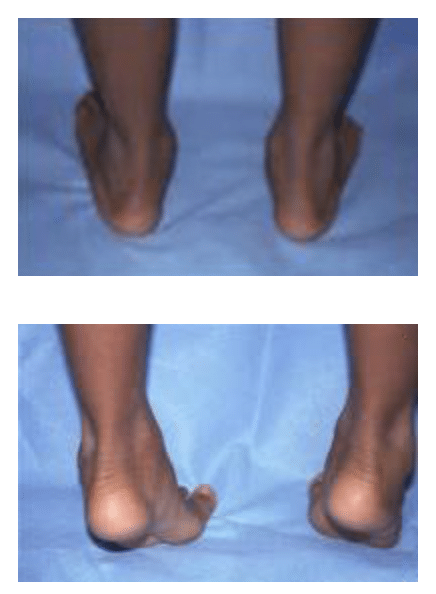
Children who do not form an arch will either develop flexible flatfeet or rigid flatfeet. To determine which type of flatfoot a child has and if any treatment is needed, the physician will examine the child’s feet, perform a neurological exam, observe their walking pattern, and may even examine the child’s shoes.
Flexible flatfeet are the most common type of flatfeet. A child with a flexible flat foot has no arch when standing, but when sitting or doing a heel rise, the arch is visible. This is due to laxity of the supporting ligaments of the arch and is often seen in children with ligamentous laxity (also known as “loose joints”).
Flexible flatfeet are rarely painful, and studies have shown that there is no long-term disability associated with flexible flatfeet. Patients with flexible flatfeet might experience pain in their foot and ankle as the get older.
Orthotics and heel cord stretching are the first line of treatment, and are usually very successful. However, there is no medical equipment nor exercise that can create an arch. For most patients with flexible flatfeet, surgery is rarely needed to relieve pain symptoms.

Rigid flatfeet are uncommon and may be due to abnormal connections between the bones in the foot. Unlike flexible flatfeet, rigid flatfoot tends to be painful as the child gets older, but symptoms can often be relieved using orthotics as the first line of treatment. If this treatment doesn’t work, surgery may be needed.
There are instances where a patient with flatfeet, flexible or rigid, will complain of pain. There are generally two pain patterns seen in people with flat feet. The first pain pattern is fatigability where a patient feels as though they can’t walk for extended periods of time. They may also have aching pain in the feet and legs, usually at the end of the day. This is usually seen in younger children and is likely due to fatigue in the leg muscles from trying to support the feet.
The second pattern is pain associated with activities and typically occurs in the morning. This is usually seen in older children and adolescents and is likely due to a tight heel cord (Achilles tendon) which limits ankle motion and puts more stress on the foot. Approximately 25% of patients with flexible flatfeet have a tight heel cord.
If a patient with flatfeet is not experiencing pain, then usually treatment is not needed. A foot cannot be forced to develop an arch, and in most cases, the flatfeet are not a problem and will not cause problems in the future.
If the child is experiencing significant pain to the point where everyday activities are impacted, then treatment options targeting the cause of the pain may be considered. Children with flexible flatfeet experiencing symptoms may be “treated” with orthotics that help support, cushion and align the foot (again, this will not develop an arch). The child should not have to wear these orthotics continously and should try to walk without them when symptoms resolve.
For patients with flatfeet and tight heel cords, stretching may be used (using orthotics with a tight heel cord often makes the pain worse). Stretching can be done at home without a therapist, or with serial casting. It’s important to pay attention to the position of the foot when stretching. The heel must be held straight or slightly inward while also keeping the knee straight to lock the hindfoot. If this method isn’t followed, the arch of the foot will be stretched instead of the ankle and may deteriorate.
Surgery is rarely considered for treating flatfeet. It is only discussed when more tradional treatments have failed (including activity modification, anti-inflammatory medication, custom orthotics, and stretching), and the patient is still reporting pain that affects their everyday life.

If surgery is considered, the doctor will explain at length what procedures take place during the operation, which includes lengthening the heel cord. The surgery takes about 3 hours and patients spend two to three days in the hospital. Afterwards, they are put into a cast and are to keep their weight off their feet for at least 6 weeks. Full recovery takes at least 6 months.