At skeletal maturity, the bones in the legs are typically equal in length and align correctly from the hips to ankles. Congenital abnormalities, infection, injury or other developmental problems however can cause limbs to grow out of alignment. This malalignment may result in deformities of the legs such as genu varum (bowlegs) or genu valgum (knock-knees), or may create a limb length inequality.
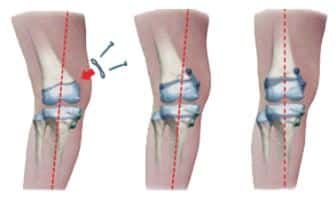
Surgery using the traditional osteotomy method is an involved procedure that requires cutting the bone, adding or removing a wedge of bone (depending on the type of deformity) and realigning the bone. The realigned bone then must be fixed with pins, a rod, or with a plate and screw combination. Correction using partial epiphysiodesis however, is a much less invasive surgical method for correcting angular deformities. Bone growth is restricted on one side of the deformity while bone growth continues on the opposite side. Gradually the bone realigns and the deformity is corrected. Since the bones are never cut with the hemi-epiphysiodesis procedure, there is less neurovascular risk, less instability, and a shorter duration of healing.
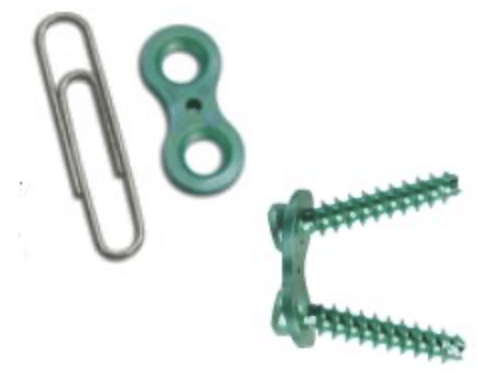
The “guided growth” plate is a unique, figure-eight shaped device about the size of a paper clip that allows gradual correction of the deformity. Common devices utilized include the Eight-Plate and the Peanut Plate.
The screws attaching the plate to the bone diverge like a hinge. This hinge action avoids too much compression on the growth plate that is being restricted. Because of the flexibility, the chances for bending or breaking the screws under the forces of bone growth are rare.
Hemi-epiphysiodesis with a guided growth device is performed under anesthesia and generally takes about an hour. During the procedure, the surgeon will make a 1” incision at the growth plate of the bone to be corrected. The titanium plate is secured to the bone with two small titanium screws. For knock-knees, the device is placed on the medial side of the bone. For bowlegs, the plate is placed on the lateral side of the bone. Multiple deformities can be addressed during the same procedure.

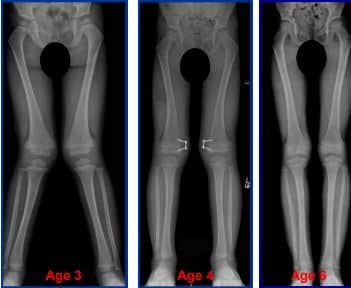
No casting is required after hemi-epiphysiodesis using a guided growth device and immediate weight bearing is encouraged. Children should be able to return to many of their normal activities within 2 to 3 weeks as comfort permits. As with any surgical procedure, pain is to be expected but should decrease during the first 2 weeks after surgery and be gone almost completely by 4 weeks after surgery. Participation in school physical education programs or sports can be resumed after consulting with the surgeon. Correction Occurs Over Time During correction the child needs to be seen by the physician about every 3 months. When the deformity is corrected, the surgeon will remove the device in an out-patient surgery setting.
A: No, the device is not meant to be permanent. It should be removed once the deformity is corrected.
A: The device may be left in as long as required to correct the deformity. Typically this is for 6 to 18 months.
A: Any regular deformity that would otherwise warrant an osteotomy, or any leg length discrepancy that would otherwise merit epiphysiodesis.
A: No, a cast is not typically required after surgery, but occasionally may be utilized.
A: Generally, patients are allowed to go home the same day– as long as no complications or other problems arise.