
Toe walking, as the name implies, describes a pattern of gait where the child walks on his or her toes. They step on the front part of their foot, and the heels do not hit the ground. Toe walking is considered normal up to age 2. Intermittent toe walking after that can be normal but persistent toe walking may merit further evaluation.
The term “idiopathic” means that the cause is unknown. Therefore, idiopathic toe walking (ITW) implies that children walk on their toes for no identifiable reason. Some common underlying causes include cerebral palsy, autism and muscular dystrophy. The first task for the physician, therefore, is to do a thorough history and physical exam to confirm that there is indeed no underlying cause. The physician will ask questions about the child’s birth history, developmental history and family history (ITW may run in families). He will then watch the child walk and perform a physical and neurological exam. Note that some underlying causes cannot be detected on routine examination.
If an underlying cause is identified, the child will be referred for further workup to the appropriate specialty. Treatment for that type of toe walking will be dependent on the cause. Some cases of neurological toe walking require treatment; others do not.
If an underlying cause is not identified then treatment may be started based on the child’s age and physical findings. There is no single right way to treat ITW, so there will be some variation depending on the patient, parents’ desires, and treating physician’s experience.
Children over 2 years of age fall into two categories of ITW: Static and Dynamic, sometimes referred to as habitual toe walking.
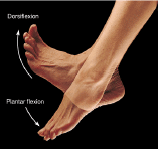
Static ITW means that there is a fixed contracture, (tightness) of the heel cord, and the child cannot dorsiflex his or her ankle enough to walk with a heel-toe pattern.
Dynamic ITW implies that the child has a normal or near normal range of motion of the ankle but prefers to walk on the toes and not the heels. For unknown reasons, this is how their brain is directing them to walk.
It should be noted that prolonged dynamic toe walking may become static toe walking over time.
There have been many treatment options described in the literature including: observation, physical therapy, stretching, botox injections, casting, bracing, surgery, and combinations of some of the above.
The first goal of treatment is to ensure the child has the range of motion necessary to walk with a heel-toe pattern. If the child has Static ITW, the contracture will need to be corrected before it is possible to walk normally.
Each child is different, and your physician will suggest the best treatment option for the child.
Physical therapy is an option but it is difficult to stretch the heel cords correctly and there is a risk for breaking down the arch of the foot. It is time intensive and costly.
Stretch casting is used if there is a mild contracture. These are fiberglass casts worn full time, typically for several weeks. The casts are changed every other week to increase the stretch.
Surgery may be needed to lengthen the heel cords if the contracture is severe. The surgery is a same-day procedure, and the child will have casts applied after the procedure while still under general anesthesia.

Once the child has good range of motion, the habit of ITW needs to be broken. Simply having the range doesn’t correct the problem as we see in children with Dynamic ITW. This is done by wearing custom molded hinged AFOs. These allow the child to walk with a heel-toe pattern, dorsiflexing the ankle but preventing toe walking. Breaking the habit may take many months. AFOs are worn as prescribed by your physician.