Tarsal coalition is a congenital abnormality where two of the bones in the back part of the foot don’t separate as they should during devel-opment and remain joined together. The cause is unknown. It can run in families and may be associated with other conditions. It is relatively uncommon and probably occurs in about 1% of the population. It affects both feet about 50% of the time and is not always symptomatic.
The cause of tarsal coalition is unknown.
Most infants and younger children do not have symptoms from tarsal coalition. This is likely due to their greater flexibility, lighter body-weight and the coalition is still made of growth cartilage and has not turned to bone (ossified) yet. Symptoms usually start to occur in the ear-ly pre-teen and teen years (9-12) for a calcane-onavicular coalition and later (12-16) for a talo-calcaneal coalition. This time also correlates with the ossification of the coalition. Symptoms may occur sooner in heavier and more active children. Most patients present with complaints of a painful flatfoot and pain with activities. Sometimes an injury such as an ankle sprain will start the symptoms. Patients may complain of recurrent “sprains”.
Physical exam may show decreased motion in the subtalar joint (side to side motion of the heel) and pain in the side or top of the foot near the ankle.
Tarsal coalitions are classified anatomically by which two bones are abnormally joined. By far the most common are Calcaneonavicular (CN) and Talocalcaneal (TC). The calcaneonavicular coalition is a connection between the calcaneus (heel bone) and the navicular. The talocalcaneal coalition is a connection between the talus (the ankle bone) and the calcaneus (heel).
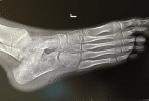
The doctor diagnoses tarsal coalition based on your symptoms, clinical examination, and x-rays. X-rays may be ordered by your doctor to confirm the diagnosis or to rule out other problems.
If the doctor suspects a coalition he will order x-rays to evaluate the foot. Plain x-rays are usually good at showing a calcaneonavicular coalition but are not good at showing a talocalcaneal coalition because of the way the bones overlap. If plain x-rays are negative the doctor may order a CT scan or an MRI of the foot to further assess for a coalition.

Treatment is based on the patient’s age and the severity of symptoms. Non-operative treatment options include: rest, activity modifications, NSAIDS and the use of an orthotic or casting.
Discontinue the activity or substitute a different activity until the pain goes away.
Taking anti-inflammatory medicine or NSAIDS (non-steroidal anti-inflammatory drugs) such as Motrin, Advil, Naproxen or Aleve as directed by your doctor can be effective. This medication should be taken for 10 to 14 days to allow the medicine to build to therapeutic levels in the body. Taking the medication infrequently allows the medicine levels to drop, which decreases effectiveness.
An orthotic or casting may be ordered by your physician to help alleviate symptoms.
If significant, life-style limiting pain returns then surgical excision (removal) of the coalition is indicated. The surgery is performed in the hospital under general anesthesia. Patients are discharged the same day in a cast or splint and use crutches, a walker or wheelchair to get around for 3-4 weeks. The cast is then re-moved and the patient is allowed to start weight bearing as tolerated in a boot or regular shoe. Full return to activities takes at least 3 months or longer depending on the extent of the surgery and patient factors.
No. There is no guaranteed method to prevent someone from developing tarsal coalition.