Once the neuromonitoring sensors are set up and all of the pre-surgery preparation is completed, we begin the surgery.

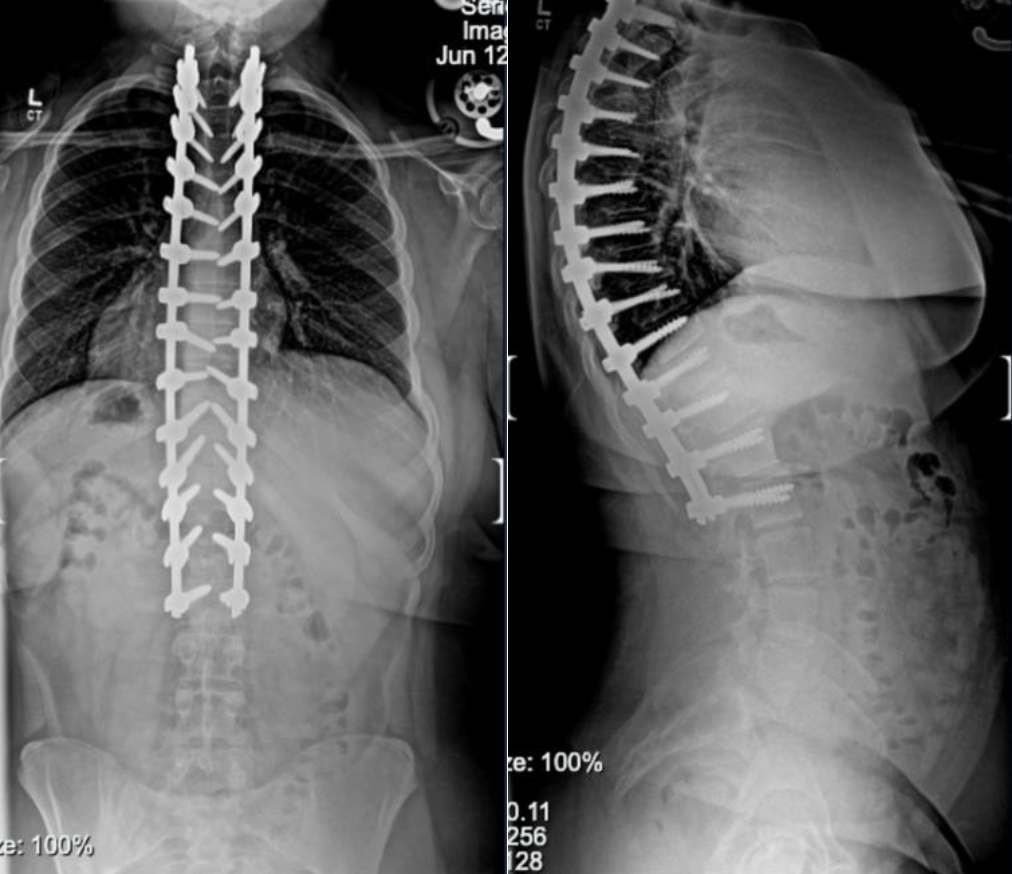
Once we are finished with the surgery, x-rays taken of your spine will show your new alignment as well as the hardware that we used.
Below are before and after photos of two of our patients who underwent a posterior spinal fusion, one for scoliosis and one for kyphosis.
Scoliosis


Kyphosis


Families are stronger when they are together. That’s why Johns Hopkins All Children’s Hospital partners with Ronald McDonald House Charities of Tampa Bay to provide the support and resources families need to stay close to their hospitalized child at little to no cost.
Johns Hopkins All Children’s offers families three Ronald McDonald Houses across campus. All locations offer private rooms, snacks, a television and laundry facilities. Some meals are provided. Hospital transport services are also available 24/7 for all locations.
A room request may be made up to 30 days in advance of a hospital stay. All adults 18 years and older must have a background check before arrival and photo ID upon arrival. To request a room at any of the houses, please call 727-767-7694.




Your child’s care team will determine when your child is ready to go home, or be discharged. Typically, they will be discharged from the hospital 1–2 days after surgery. However, their discharge date will depend on their progress throughout their hospital stay.
In order to go home, your child must achieve the following:
We will prescribe your child several medications for them to take at home to keep their pain under control. These will be the same medications they were taking while in the hospital.
A parent or legal guardian will need to be present to take your child home if they are under the age of 18. If your child is over 18, they will need to arrange for someone to accompany them home. They will not be released without someone present.
When your child is leaving the hospital, you will receive an After Visit Summary (AVS). This document includes information about your child’s surgery, incision care, pain management, activity level, diet, home care, and other important instructions.
Call your surgeon’s office anytime if you are worried about your child’s recovery. During regular office hours (9:00 a.m. – 5:00 p.m.), call your surgeon’s office directly. After hours, our main office number will connect you with an answering service, who will then connect you with the orthopaedic PA or resident on call.
Call your surgeon’s office immediately if:
After surgery, your child will have a bandage in place over their incision called Aquacel Ag.
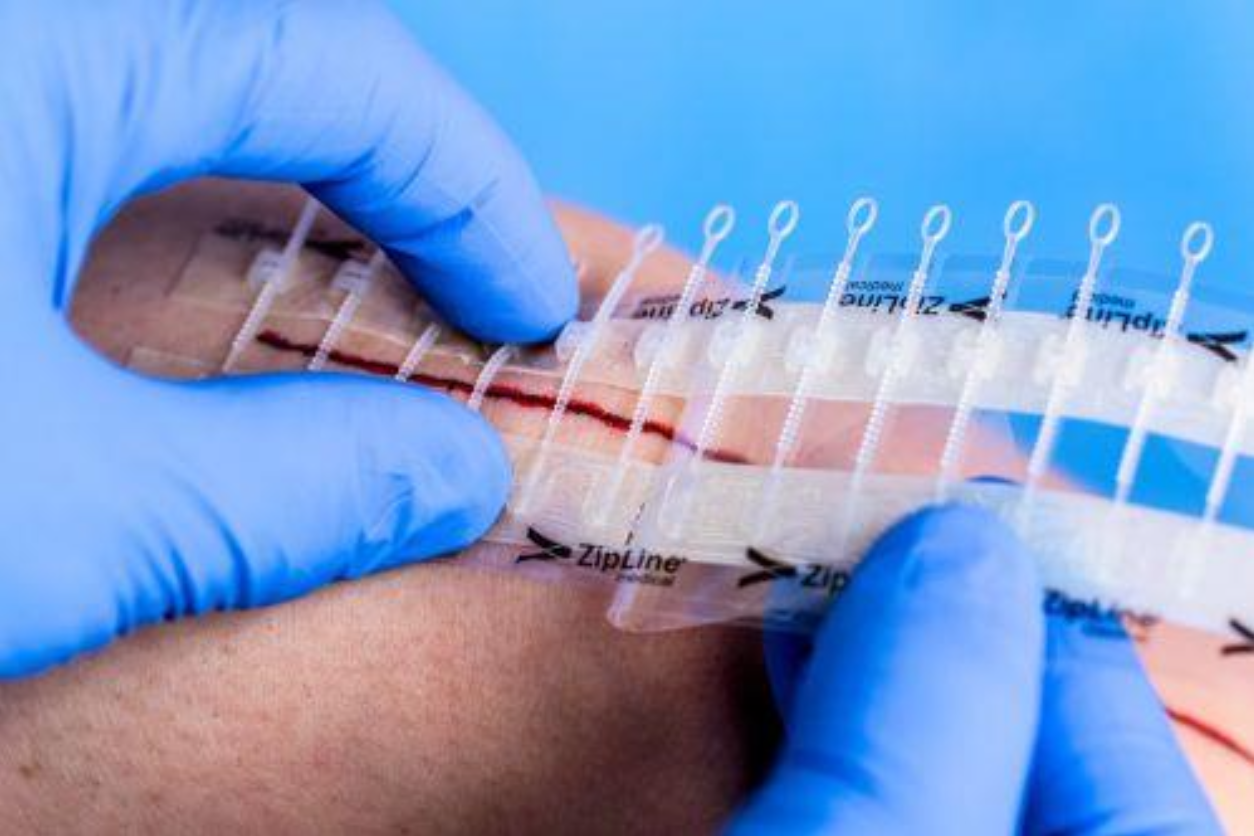
Ten days after your child is discharged, you may remove the Aquacel Ag dressing and ZipLine dressing at home.
You should protect the incision from the sun for the first year after surgery. We recommend using sunscreen with SPF 45 or higher or UV-protective clothing to cover the incision. The more tanned or sunburned the scar becomes, the less likely it is to return to a normal skin tone. Do not apply any creams, lotions, or oils until cleared by your surgeon.
Once cleared by your surgeon, your child may use topical creams on their incision if desired. We recommend using silicone scar bandages to help the scar heal. These can help collagen fibers realign more effectively and are available online. One brand we often use is Nuvadermis.
It is very normal for the sensation around your child’s incision to be decreased or overly sensitive after surgery. This may include numbness, hypersensitivity, or reduced sensation. These changes can be limited to the incision area or extend across a larger portion of the back. Sensations usually improve gradually over the first few months but may take up to two years. Most patients experience mild residual numbness or decreased sensation directly over the incision that may never fully resolve.



It is very important that your child follows all of the activity restrictions that were given to you. Doing too much too quickly can cause problems such as their incision reopening or their hardware breaking, both of which could require a second surgery. Below is a general list of when your child may begin doing certain activities. Do not resume any of these activities until their surgeon has cleared them. If you have questions about any specific activities, please ask your surgeon.
Following surgery, your child’s first post-op appointment will be 2–3 weeks after the surgery date. This appointment should already be scheduled prior to your surgery day.
After that, your child will have appointments at the following intervals:
After the 2-year post-op appointment, no further appointments will need to be scheduled. We will always be happy to see your child in the office for any problems, concerns, or questions.
People have a variety of emotions when facing a major surgery. This is true for both parents and the child having surgery. It is good to look to others for support. Oftentimes family, friends, and people from church will offer to help when they know a loved one is going through a major event. Think of ways you can take them up on that offer to help, such as preparing meals, staying at your home with the other children or pets, or coming to your home to stay with your child while you rest or run errands. Families cope in different ways—time with family and friends, time alone, humor, prayer, communion with nature, meditation, journaling, art, and music.
Some patients and parents find it helpful to connect with another family who has been through the same surgery. We have a list of patients and their families who have gone through spinal fusion surgery and have offered to speak with others about their experience. If you would like to speak with any patients or their families, please notify our office and we will be happy to provide you with contact information.
If you would like to volunteer to share your experience after surgery, please let one of our surgical coordinators know so they can add you to the list.
As your child is recovering at home, we strongly recommend that they take all of their prescribed medications as scheduled instead of waiting for discomfort to return before taking the next dose. When taken on schedule, medications help your child “stay ahead of the pain.” It is much harder to control discomfort once they are already in pain and trying to catch up. As their discomfort improves over the first week or two, they may gradually begin increasing the time between doses.
Note: Please remember that your child just had major spine surgery. While they may not like the idea of taking narcotics and muscle relaxers, these medications are integral to keeping them comfortable during the first week or two of recovery. If they opt not to take them and their discomfort becomes too severe, it will take time to get their pain back under control.
Why is my child having pain in their neck and shoulders?
It is common to experience some discomfort in the neck and shoulders after surgery. The spine is now in a position it is not used to, and the muscles need to adjust to this new alignment. This can lead to muscle pain in the back, neck, and shoulders. Your child should continue with their prescribed pain medications. Once the incision is healed, heat and light massage may also help with neck and shoulder discomfort.
Why does my child have pain or tingling in their thighs?
Some patients report numbness, tingling, or a “burning” pain in the front of their thighs after surgery. This is due to compression on the femoral cutaneous nerve and can be a common side effect. Do not worry—this is temporary and will improve on its own with time. It is not associated with muscle weakness or numbness anywhere else in the legs. However, if your child experiences muscle weakness or numbness in any other part of their legs, ple
It can be normal to have a small amount of drainage from your child’s incision after they go home. You may notice this drainage on the dressing. However, if there is so much drainage that it seeps through the sides of the dressing or drips from the bottom, please contact our office right away.
If the drainage or the incision begins to cause increased pain or develops a foul odor, contact our office immediately. If your child develops redness or the wound begins to open, please take a picture and email it to our nursing staff through the patient portal. Please see page 27 for their contact information.
For instructions on your post-op dressing, please refer to page 19.
After surgery, your child may become constipated for a number of reasons:
If this should happen, here are some solutions to help:
Some patients are discharged from the hospital with a portable wound vac. A wound vac uses Negative Pressure Wound Therapy to help hold the edges of the incision together and improve wound healing.
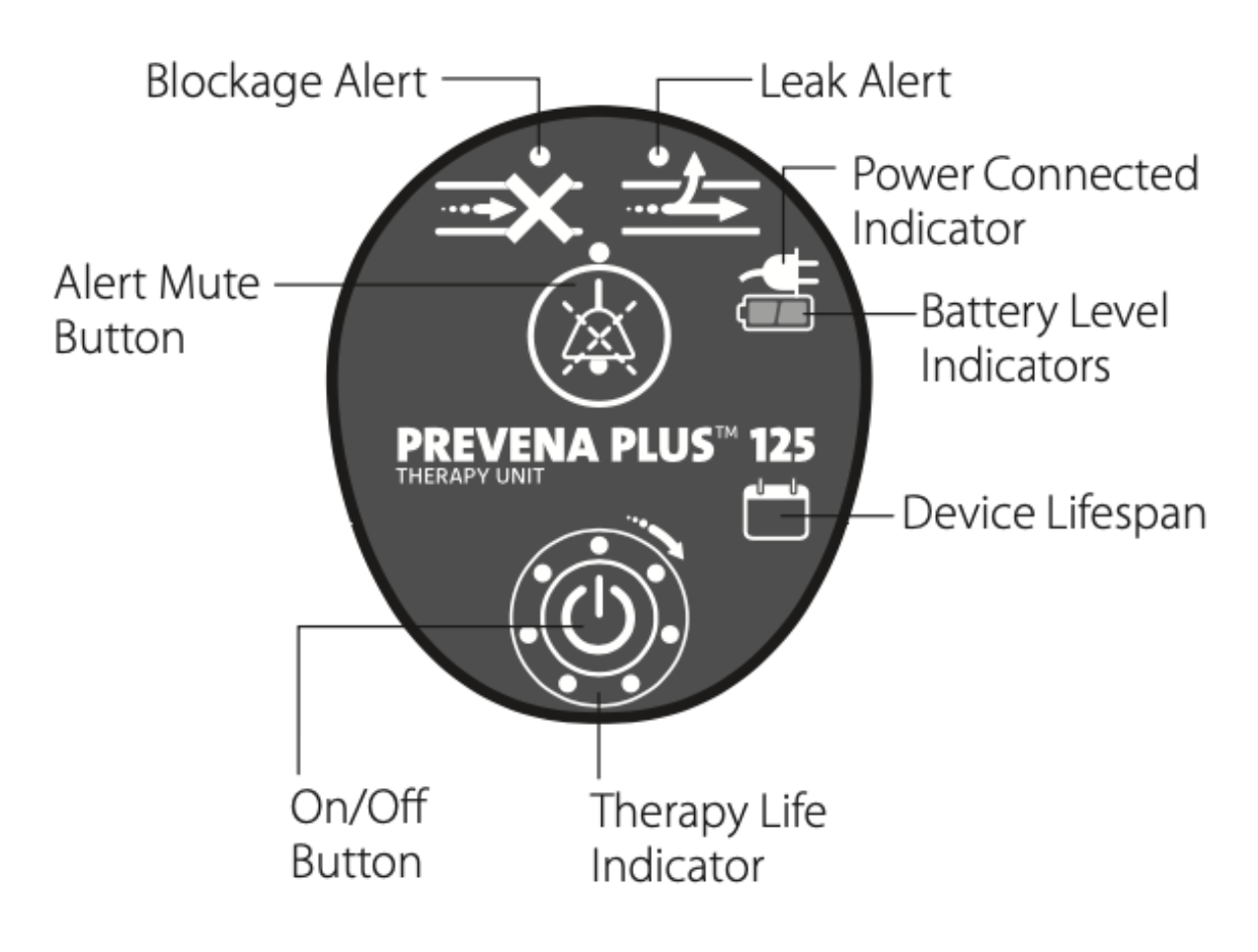
The unit has several indicator lights on the front that can alert you if there is a problem. There will typically be a beeping sound associated with one of the indicator lights turning on. The image to the right demonstrates what each indicator light means.
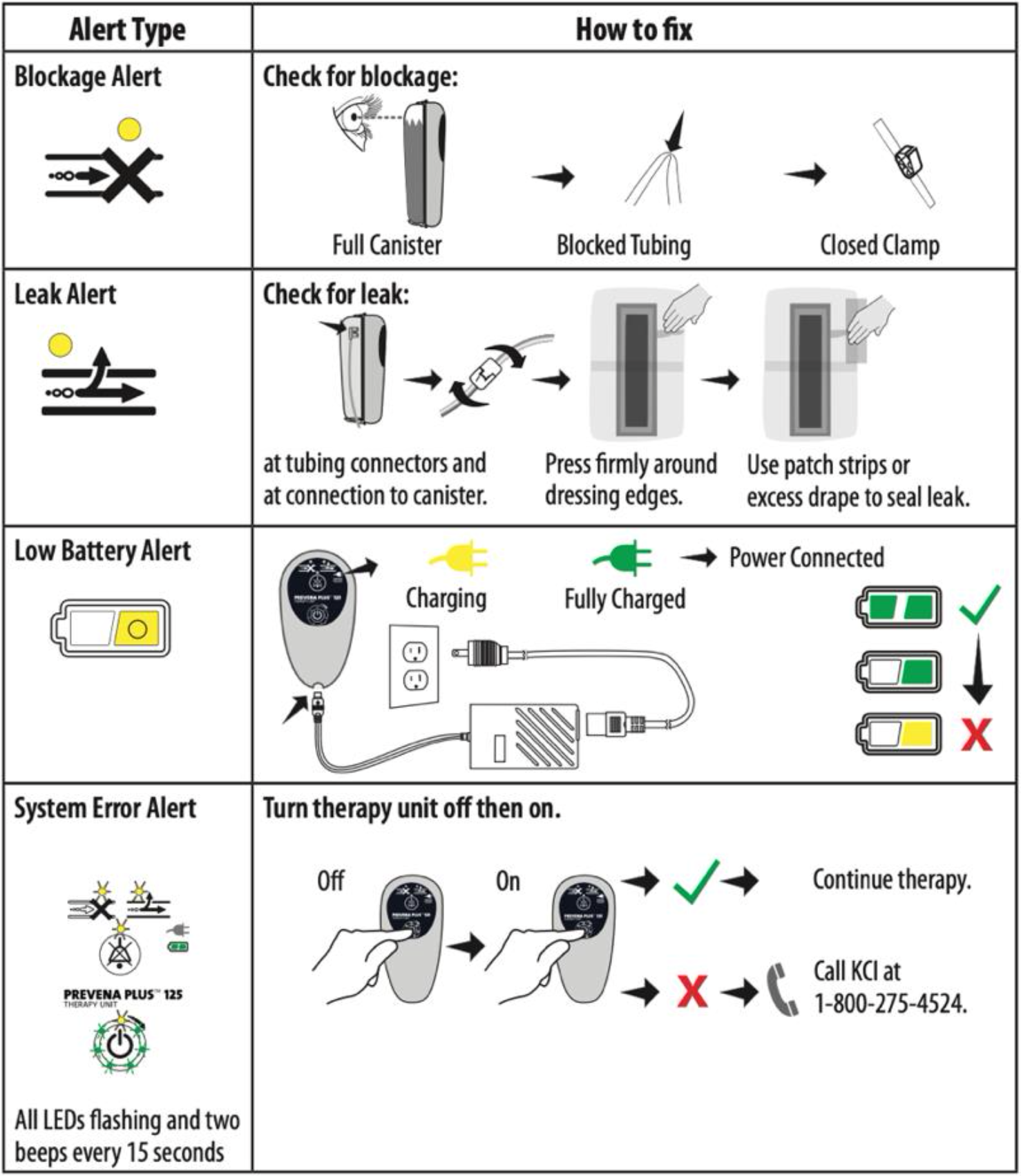
There are several simple things you can do at home to troubleshoot any problems you may have with your child’s wound vac.
If there is a block: Check that the tubing is not kinked and that the clamp is open. You may also get this warning if the canister is full. If the canister is full or almost full, please contact our office right away.
If there is a leak: Check that the tubing is properly plugged in. Examine the dressing for any edges that may have peeled back or any places where air may be leaking out. If the dressing is leaking air, you can reinforce any areas of leak with the extra dressings you were provided at discharge.